
For many patients, the most exhausting symptom of their condition isn't the racing heart, but the persistent suggestion that they are simply anxious. It's a frustrating reality that the average diagnostic delay for Postural Orthostatic Tachycardia Syndrome (PoTS) is five years or more, often because physical symptoms are mistaken for a psychological disorder. You've likely felt the sting of being dismissed when your heart hammers in your chest just by standing up, only to be told you need to manage your stress whilst your physical symptoms continue to disrupt your daily life. Understanding the difference between pots and anxiety is the first step toward reclaiming your health and ensuring you receive the precise clinical care you deserve.
I agree that feeling your body fail you is inherently stressful; however, that doesn't mean your mind is the primary cause of your tachycardia. This guide will provide the clarity you need to validate your experience and explain the physiological mechanisms at play, ensuring you understand exactly which tests are required for an accurate diagnosis. We'll examine the diagnostic role of the active standing test and how a clinical assessment by a consultant cardiologist like Dr Ayyaz Sultan can help distinguish cardiovascular dysfunction from psychological worry.
Key Takeaways
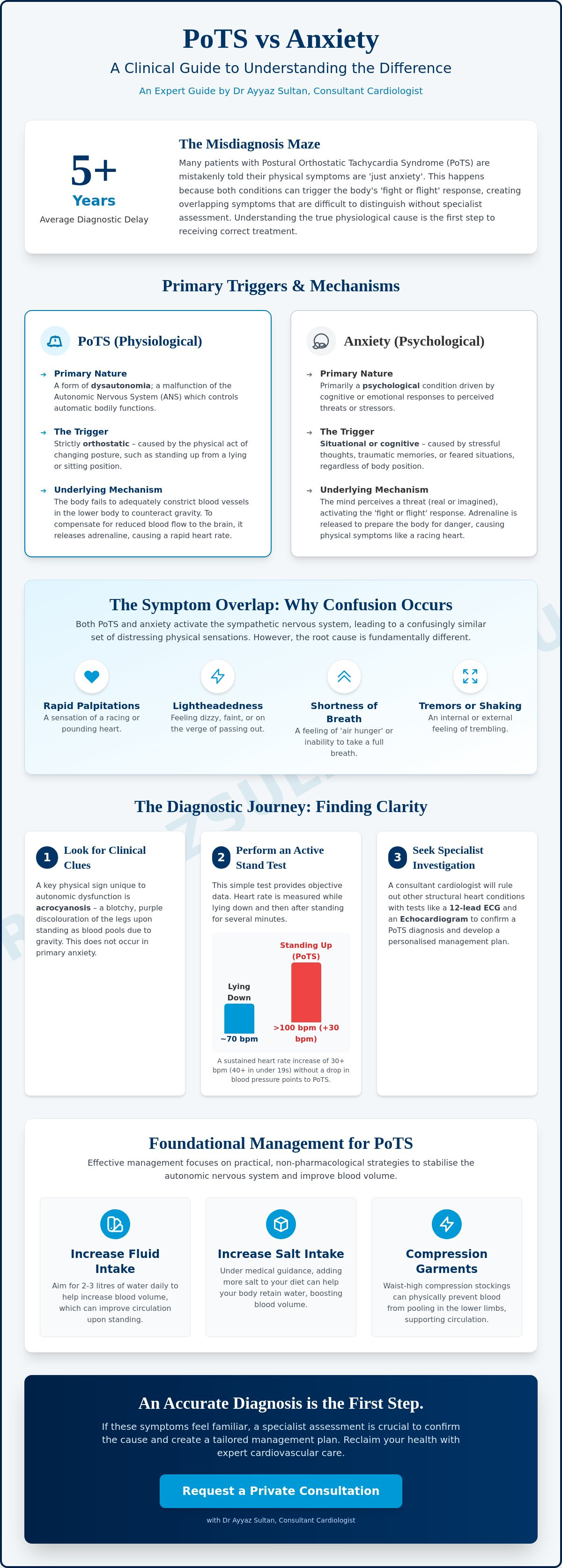
- Understand why PoTS is a physiological form of dysautonomia triggered by postural changes, whereas anxiety is primarily driven by cognitive or situational stressors.
- Learn how the Active Stand test provides objective clinical data to establish the difference between pots and anxiety by measuring heart rate responses to gravity.
- Identify physical indicators unique to autonomic dysfunction, such as acrocyanosis (purple discolouration of the legs), which do not occur in primary psychological conditions.
- Discover the essential role of specialist investigations, including a 12-lead ECG and private cardiac consultation, in ruling out structural heart disease and confirming a diagnosis.
- Explore practical, non-pharmacological management strategies like increased hydration, salt intake, and compression garments to help stabilise your autonomic nervous system.
The Misdiagnosis Maze: Why PoTS is Frequently Mistaken for Anxiety
Patients seeking answers for a racing heart often find themselves caught in a cycle of clinical dismissal. It's a sobering reality that many individuals living with Postural orthostatic tachycardia syndrome (PoTS) face a diagnostic delay of five years or more. During this time, their physical distress is frequently labelled as a psychological issue. This misidentification occurs because both conditions trigger the body's "fight or flight" response, creating a confusing overlap of physiological signals that can baffle even experienced general practitioners.
When the heart rate spikes and breath becomes shallow, the brain naturally interprets these signals as danger. For a patient with PoTS, this isn't a reaction to a stressful thought, but a physical failure of the body to regulate itself against the pull of gravity. As a consultant cardiologist, Dr Ayyaz Sultan often sees how this misdiagnosis leads to inappropriate treatments and profound patient distress. Distinguishing the difference between pots and anxiety requires a meticulous clinical approach, as psychological interventions cannot fix a physiological autonomic malfunction.
To better understand this concept, watch this helpful video:
What is PoTS? An Autonomic Nervous System Perspective
The Autonomic Nervous System (ANS) is the body's internal autopilot. It manages everything from your digestion to your heart rate without you ever having to think about it. In a healthy system, standing up triggers a swift and coordinated response where blood vessels in the lower body constrict to push blood upward against gravity. In PoTS, this mechanism falters. Instead of efficient vasoconstriction, the body compensates for the lack of blood flow to the brain by releasing a surge of adrenaline, causing the heart to race. This is a purely physiological condition, a form of dysautonomia, rather than a primary mental health disorder.
The Overlap: Shared Symptoms That Cause Confusion
The difference between pots and anxiety is often clouded by the fact that they share a nearly identical symptom profile. When the sympathetic nervous system is overactive, patients frequently experience:
- Rapid palpitations and chest discomfort.
- Shortness of breath or "air hunger".
- Lightheadedness and near-fainting, known as presyncope.
- Tremors and a feeling of internal "shaking".
It's entirely understandable why a medical professional might initially suspect a panic attack. However, the physical sensation of a racing heart can itself generate a sense of doom or secondary anxiety. Validating that these symptoms have a physical origin is a crucial step in the patient journey. Experiencing a heart rate that jumps by 30 beats per minute just by standing is genuinely distressing. Recognising this as a cardiovascular event rather than a worry-based reaction is essential for correct management and long-term recovery.
Understanding the Mechanism: Autonomic Dysfunction vs Psychological Stress
To truly grasp the difference between pots and anxiety, we must look beyond the symptoms and examine the underlying triggers. Anxiety is typically cognitive or situational; it is a response to a perceived threat, a stressful thought, or a traumatic memory. In contrast, Postural Orthostatic Tachycardia Syndrome is strictly orthostatic. This means the primary trigger isn't a worry, but the simple physical act of standing up and the subsequent pull of gravity on the circulatory system.
As Dr Ayyaz Sultan often explains to his patients, PoTS is a form of dysautonomia, which is a systemic failure where the autonomic nervous system cannot properly manage involuntary functions like blood flow. For those with Hyperadrenergic PoTS, the body overproduces norepinephrine, a potent stress hormone, as a desperate attempt to constrict blood vessels that aren't responding. When the brain detects a drop in blood pressure or oxygenation, it sends an emergency signal to the heart. This creates a physiological feedback loop where the brain interprets physical instability as psychological panic, leading many patients to feel a sense of dread that is actually rooted in their cardiovascular system. This is why the difference between pots and anxiety is so frequently misunderstood in general practice.
The Adrenaline Connection: Why You Feel "Wired and Tired"
When you stand, your body may dump a surge of adrenaline (epinephrine) into your bloodstream to force your heart to work harder. This results in a "wired but tired" sensation that is common amongst dysautonomia patients. You might feel jittery, shaky, and hyper-alert, yet physically exhausted. Crucially, this surge can occur whilst you're mentally calm, perhaps just standing in a queue or brushing your teeth. It isn't a panic attack born of cognitive stress; it's an involuntary autonomic reflex that leaves you feeling drained for hours after the initial spike.
Blood Pooling and the Gravity Factor
Gravity is a constant force that pulls blood toward your lower limbs and abdomen. In a healthy individual, the body counters this immediately through vasoconstriction. In PoTS, blood pools in these lower areas, leaving the heart to beat faster and harder to keep the brain oxygenated. Anxiety doesn't require a change in posture to manifest, but PoTS is defined by it. If you find your heart rate only settles when you lie down, it's a strong indicator that your symptoms are physiological. If you're struggling to untangle these sensations, you may wish to book a specialist assessment to receive a clear, data-driven diagnosis.
Key Clinical Differences: How to Distinguish PoTS from Panic
Distinguishing the difference between pots and anxiety requires moving beyond patient history and into objective clinical observation. The most definitive tool available is the Active Stand Test, which can often be conducted during an initial private consultation. To meet the diagnostic criteria for PoTS, an adult must exhibit a sustained heart rate increase of 30 beats per minute (bpm) or more within ten minutes of standing. This must occur in the absence of orthostatic hypotension, which is a significant drop in blood pressure. For adolescents aged 12 to 19, the required increase is 40 bpm or more.
Whilst anxiety may cause tachycardia, the heart rate does not typically follow this rigid postural pattern. Physical examinations often reveal acrocyanosis, a distinct mottled or purple discolouration of the lower legs caused by blood pooling. This physical sign is a hallmark of autonomic dysfunction and is entirely absent in psychological panic disorders. By focusing on these measurable physiological markers, Dr Ayyaz Sultan can provide patients with the clinical evidence needed to move past a misdiagnosis of anxiety.
The Positional Trigger: The Defining Feature
The defining feature of PoTS is its relationship with gravity. Symptoms typically resolve or improve significantly once the patient lies down, as the heart no longer has to fight the downward pull of blood to oxygenate the brain. This positional nature explains why many patients feel their worst in the morning, when blood volume is at its lowest, or after a hot shower, which causes blood vessels to dilate and worsens pooling. Panic attacks, however, are not governed by your physical orientation. They can occur whilst you are lying in bed or sitting perfectly still, often triggered by internal thoughts or external stressors rather than the act of standing.
Associated Physical Findings in PoTS
Dr Ayyaz Sultan often evaluates patients for what is known as the "PoTS Triad", a complex intersection of PoTS, Joint Hypermobility (such as hEDS), and Mast Cell Activation Syndrome (MCAS). These associated conditions provide further evidence of a physiological cause. Patients may report non-cardiac symptoms like temperature intolerance, excessive sweating, or gut motility issues, which suggest a broader systemic failure of the autonomic nervous system. Identifying these multi-system markers is vital in establishing the difference between pots and anxiety, as they point toward a complex physiological syndrome rather than a primary mental health concern.
The Diagnostic Journey: Moving Beyond a Mental Health Diagnosis
Moving from the frustration of unexplained symptoms to a definitive clinical diagnosis is a pivotal moment in any patient's journey. A private cardiac consultation with an experienced specialist like Dr Ayyaz Sultan is essential to move beyond a mental health label. This process isn't just about identifying PoTS; it's about systematically ruling out structural heart disease or other underlying rhythm disturbances that might mimic the condition. Relying on a general assessment often leads to a cycle of misdiagnosis, as the nuances of autonomic dysfunction require a high degree of cardiovascular expertise.
The diagnostic process typically begins with a standard 12-lead ECG to assess your baseline heart rhythm and ensure there are no electrical abnormalities. A significant hurdle for many patients is that routine blood tests for thyroid function, iron levels, and basic metabolic markers often come back entirely "normal." Whilst these tests are necessary to exclude other causes of fatigue and palpitations, they cannot detect the autonomic instability that defines PoTS. This lack of visible abnormality in routine screening is a primary reason why the difference between pots and anxiety is frequently overlooked in primary care settings.
To support your clinical evaluation, I recommend maintaining a detailed diary of your heart rate and blood pressure. Recording these measurements whilst lying down, immediately upon standing, and after ten minutes of standing provides a clear data set. This self-tracking helps identify the specific postural patterns that distinguish a physiological condition from situational worry.
The Gold Standard: Tilt Table Testing
When an active stand test in the clinic is inconclusive, a Tilt Table Test may be recommended. During this procedure, you are secured to a specialised table that moves from a horizontal to a nearly vertical position whilst your heart rate and blood pressure are continuously monitored. This test is designed to isolate your body's orthostatic response by removing the "muscle pump" action of the legs that occurs during normal standing. A positive diagnosis in adults is confirmed by a sustained heart rate increase of 30 beats per minute or more within ten minutes of being tilted, providing the objective evidence needed to validate your physical experience.
Ambulatory ECG and Holter Monitoring
Whilst a standard ECG captures only a few seconds of heart activity, a 24-hour or 7-day Holter monitor records your heart's behaviour throughout your normal daily routine. These ambulatory monitors are vital for capturing "symptom-events," such as a spike in heart rate whilst you are performing simple tasks like making a cup of tea. This data allows a cardiologist to confirm that your racing heart is a sinus tachycardia (a normal rhythm that is simply too fast) triggered by posture, rather than a primary arrhythmia or a panic attack. If you are seeking clinical clarity for your symptoms, you can book a comprehensive cardiac assessment to begin your diagnostic journey.
A Holistic Approach to Managing PoTS and Co-existing Anxiety
The difference between pots and anxiety becomes most apparent during the treatment phase. When a patient is told their symptoms are "just stress," the lack of physical relief often causes their mental health to spiral, creating a secondary layer of genuine anxiety. Validating that your symptoms are rooted in autonomic dysfunction is a powerful clinical tool. It shifts the focus from "fixing a worry" to stabilising a system. Once you understand that your racing heart is a physical response to gravity, the psychological burden of uncertainty begins to lift, allowing for a more focused recovery.
Effective management starts with universal non-pharmacologic strategies. I often advise patients to significantly increase their fluid and salt intake to expand blood volume, alongside the use of medical-grade compression garments to reduce blood pooling in the lower limbs. These simple adjustments provide a foundation of stability that psychological therapy alone cannot achieve. When these measures aren't enough, specialised cardiology services can provide tailored pharmacological support. Medications such as beta-blockers or ivabradine are frequently used to lower the heart rate and improve exercise tolerance. It's a common clinical observation that as the physical tachycardia is controlled, the "anxiety" symptoms often vanish entirely, proving they were a symptom of the condition rather than the cause.
Personalised Treatment Plans by Dr Ayyaz Sultan
Dr Ayyaz Sultan advocates for a patient-centred approach that recognises the complexity of multi-system conditions. Every individual's autonomic profile is unique, requiring a management plan that balances modern medicine with realistic lifestyle strategies. A multidisciplinary view is essential for success. This might involve coordinating with specialists in hypermobility or nutrition to address the underlying drivers of your dysautonomia. This holistic framework ensures that we aren't just treating a heart rate, but supporting the whole person on their journey toward long-term recovery and improved daily function.
Next Steps: Booking Your Private Assessment
If you feel your symptoms have been dismissed or if you're struggling to find a clear path forward, seeking an expert opinion is the next logical step. You don't have to navigate this complex condition without guidance. A correct diagnosis is the vital first step towards reclaiming your quality of life and moving past the confusion of misdiagnosis. You can book an Initial Private Consultation to discuss your symptoms in a supportive, expert-led environment where your experiences are heard, validated, and investigated with clinical precision.
Reclaiming Your Quality of Life through Clinical Clarity
Navigating the path to an accurate diagnosis requires a fundamental shift from managing worry to investigating physiology. You now understand that PoTS is a systemic failure of the autonomic nervous system, defined by its specific relationship with gravity rather than a psychological disorder. Recognising the difference between pots and anxiety is the essential first step in ensuring your symptoms are validated and treated with the clinical precision they require.
Dr Ayyaz Sultan has served as a Consultant Cardiologist since 2013, specialising in the complex intersections of PoTS and autonomic dysfunction. His approach combines high-level clinical authority with deeply empathetic, patient-centred care, ensuring that your physical experiences are never dismissed. By prioritising data-driven diagnostics over vague labels, he helps patients build a sustainable framework for recovery and long-term health.
If you're ready to move from confusion to a clear management plan, you can Book a Private Cardiac Consultation with Dr Ayyaz Sultan today. You deserve a diagnostic journey that respects your experience and provides the answers you need to move forward with confidence.
Frequently Asked Questions
Can PoTS feel exactly like a panic attack?
PoTS can mimic the physical sensations of a panic attack almost perfectly because both conditions involve a significant surge in the sympathetic nervous system. You may experience a racing heart, tremors, and shortness of breath that feel identical to a psychological crisis. The key distinction is that PoTS symptoms are triggered by the physical act of standing, whereas panic attacks are usually independent of your posture.
Is it possible to have both PoTS and an anxiety disorder simultaneously?
It is certainly possible to live with both conditions, as the burden of a chronic physical illness can naturally lead to secondary mental health challenges. Understanding the difference between pots and anxiety is crucial in these cases; one is a failure of autonomic regulation whilst the other is a psychological response. Treating both requires a multidisciplinary approach that addresses the cardiovascular system and the mind as separate but related entities.
Why do doctors often misdiagnose PoTS as anxiety?
Misdiagnosis occurs because many clinicians focus on the symptoms, such as palpitations and sweating, rather than the triggers. These are classic markers of anxiety, and without performing a postural heart rate check, it is easy to overlook the orthostatic nature of the condition. Dr Sultan often finds that patients are dismissed because their standard resting ECG and blood tests appear normal, leaving the autonomic dysfunction undetected.
How can I tell if my racing heart is caused by stress or PoTS?
The most reliable way to distinguish the two is to observe exactly when the symptoms occur. If your heart races primarily when you are upright and settles almost immediately when you lie down, it points toward a physiological cause like PoTS. If the racing heart happens regardless of whether you are sitting, standing, or lying down, it may be more closely linked to situational stress or a primary heart rhythm disturbance.
What is the "Stand Test" and can I do it at home?
The Active Stand Test involves measuring your heart rate and blood pressure after lying flat for five minutes and then again at intervals after standing still for ten minutes. Whilst you can perform this at home to gather data for your GP, a formal diagnosis should be confirmed in a clinical setting. This ensures that confounding factors, such as current medications or acute dehydration, are professionally evaluated by a specialist.
Does PoTS go away if I treat my anxiety?
No, treating anxiety will not resolve the underlying autonomic dysfunction that causes PoTS. Whilst reducing stress can help you cope with the challenges of chronic illness, PoTS is a physical condition that requires physiological interventions like salt loading, hydration, and compression. The difference between pots and anxiety is that one is a "software" issue of the mind, whilst the other is a "hardware" malfunction of the nervous system.
What should I do if my GP says my symptoms are just stress?
If your GP attributes your symptoms to stress, you should calmly advocate for an objective assessment of your cardiovascular response to posture. Ask specifically for an Active Stand Test to be performed in the surgery to document your heart rate changes. If you continue to feel dismissed, seeking a private consultation with a cardiologist who understands dysautonomia can provide the clinical clarity and validation you deserve.
Can adrenaline surges in PoTS cause feelings of panic?
Adrenaline surges are a core component of Hyperadrenergic PoTS and can create an intense feeling of internal jitteriness, shaking, or dread. These norepinephrine spikes occur because the body is overcompensating for poor blood vessel constriction. It is important to recognise that these feelings are a direct physical byproduct of your autonomic nervous system's struggle to maintain blood flow, rather than a sign of a psychological panic disorder.