
What if the reason your blood pressure remains stubbornly high isn't a failure of your willpower, but a missing piece of a complex physiological puzzle? It's a common and deeply frustrating experience to take three or more medications exactly as prescribed, only to find your readings still refuse to budge below the recommended 130/80 mmHg target. You might feel a sense of failure or fear the silent damage occurring within your heart and kidneys, especially when home readings clash with those taken in the clinic.
Dr Ayyaz Sultan, an experienced Consultant Cardiologist, understands that understanding what is resistant hypertension is the first step toward a solution. This condition is often a diagnostic signal rather than a treatment dead-end. In this guide, we'll explore why some blood pressure resists standard care and how a meticulous, specialist-led approach can uncover underlying secondary causes. You'll gain a clear clinical explanation for your resistance and a reassuring roadmap for the investigations, such as ambulatory monitoring or specialist imaging, needed to finally restore your health and peace of mind.
Key Takeaways
- Understand the specific clinical criteria for what is resistant hypertension, including why a diuretic must be part of your three-medication regimen to meet this diagnosis.
- Learn how to distinguish between genuine treatment resistance and "pseudo-resistance" caused by factors like the white coat effect or inconsistent measurement techniques.
- Discover the vital role of 24-hour Ambulatory Blood Pressure Monitoring (ABPM) in providing the precise data Dr Ayyaz Sultan needs for a specialist evaluation.
- Recognise the long-term risks of uncontrolled pressure, such as heart muscle strain, and why a consultant-led approach is necessary to protect your vascular health.
- Explore personalised management options, from investigating hidden secondary causes to optimising the timing of your doses through chronotherapy.
Defining Resistant Hypertension: When Standard Treatment Isn't Enough
For many patients, the daily ritual of swallowing multiple tablets can become a source of quiet anxiety rather than a path to health. You've followed the medical advice, changed your diet, and yet the monitor still flashes red. This "pill fatigue" is real. It's not just about the numbers; it's about the feeling that your body isn't responding as it should, which can lead to a sense of frustration or even defeat.
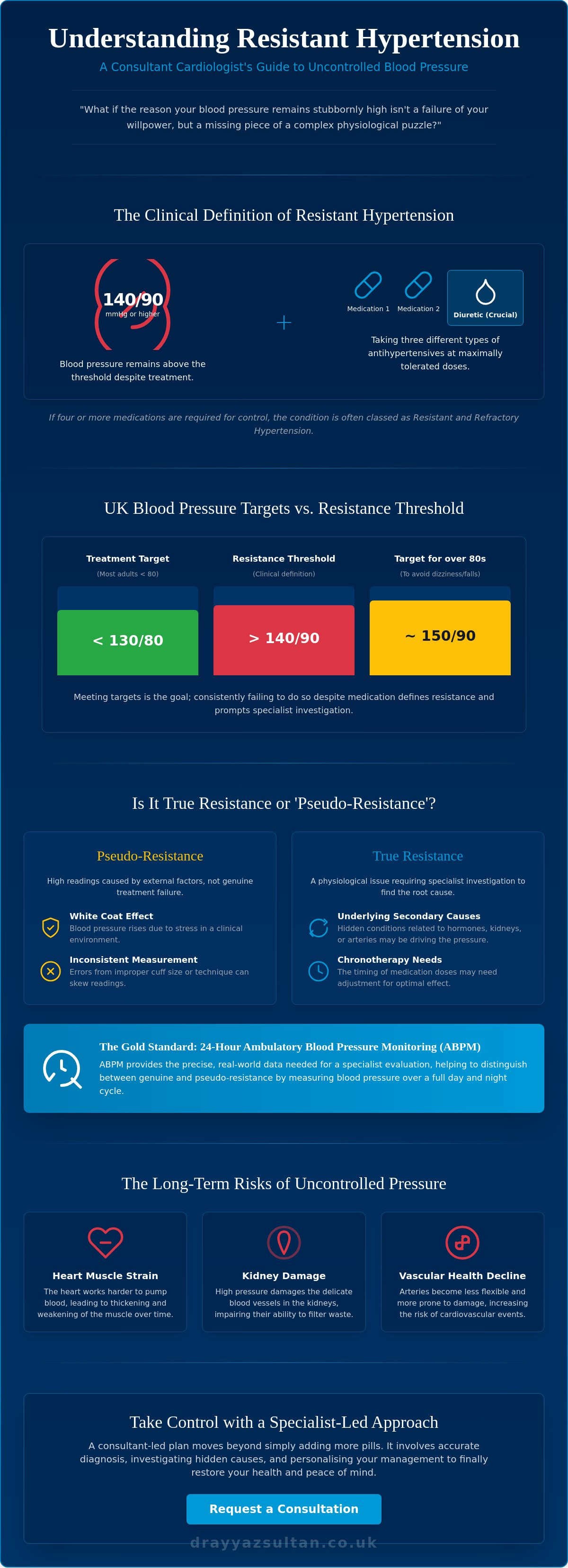
Understanding what is resistant hypertension involves looking at specific criteria used by expert cardiologists like Dr Ayyaz Sultan. It isn't simply "high blood pressure" that's a bit high. It's a clinical signal that the standard primary care approach has reached its limit. To be diagnosed, your blood pressure must remain above 140/90 mmHg whilst you're taking three different classes of antihypertensive medication at their maximally tolerated doses. Crucially, one of these three must be a diuretic. Without a diuretic in the mix, we can't definitively say the pressure is "resistant" because fluid retention often remains a hidden driver of uncontrolled readings.
To better understand this concept and how it's managed, watch this helpful video:
The 'Three-Medication' Threshold
The logic behind combining medications like ACE inhibitors, Calcium Channel Blockers (CCBs), and Thiazide-like diuretics is to target different physiological pathways simultaneously. By addressing the kidneys, blood vessels, and hormonal systems at once, we usually expect to see a significant drop in pressure. When this doesn't happen at "maximally tolerated doses"—the highest dose you can take without side effects—it suggests an underlying complexity. According to the 2026 UK clinical criteria, resistant hypertension is defined as a clinic blood pressure of 140/90 mmHg or higher despite the use of three antihypertensive drugs including a diuretic. If you require four or more medications to achieve control, the condition is often categorised as Resistant and Refractory Hypertension. Identifying what is resistant hypertension early is vital because it shifts the clinical focus from simply lowering numbers to finding the hidden 'why' behind the resistance.
UK Blood Pressure Targets and NICE Guidelines
NICE guidelines emphasise that clinic readings are often higher than home measurements due to the "white coat effect," where the clinical environment itself raises a patient's stress levels. For most adults under 80, the universal treatment target is now less than 130/80 mmHg, although the threshold for defining resistance remains 140/90 mmHg. For those over 80, targets are slightly higher, typically around 150/90 mmHg, to avoid the risks of dizziness or falls. Precision is key here. It's also recognised that resistant hypertension is more common in males and adults over 75, making these age-specific targets even more critical. When these targets aren't met at Step 4 of the British healthcare framework, it's a clear prompt for a specialist cardiology investigation. Rather than simply adding more pills, Dr Sultan focuses on uncovering why the current regimen isn't working, ensuring your care is personalised and effective.
Uncovering the Causes: Why Your Blood Pressure Remains High
When your blood pressure remains high despite multiple medications, the first step in a specialist review is to determine if the resistance is "true" or "apparent." This distinction is vital because it changes our entire management strategy. Identifying what is resistant hypertension requires a meticulous process of elimination, looking beyond the numbers to see if there's an external factor or an underlying medical condition driving the elevation. It's about finding the "why" rather than just accepting the "is."
Pseudo-resistance and Measurement Errors
It's estimated that "White Coat Hypertension"—where readings are elevated only in a clinical setting due to anxiety—accounts for up to 30% of cases that appear resistant. This is why Dr Sultan often recommends ambulatory monitoring to capture your pressure in your natural environment. Beyond nerves, the "Cuff Effect" is a common culprit; if a blood pressure cuff is too small for your arm, it can provide a falsely high reading. We also approach medication non-adherence with deep empathy. Managing four or five different tablets a day is a significant burden, and it's understandable when doses are missed or timing becomes inconsistent. Understanding these Clinical Findings in Resistant Hypertension helps us differentiate between a need for more medication and a need for better measurement or adherence support.
The Role of Secondary Medical Conditions
In many instances, high blood pressure is a symptom of another issue elsewhere in the body. Primary Aldosteronism is a common secondary cause where the adrenal glands produce an excess of aldosterone, a hormone that causes the body to retain salt and lose potassium. Other patients may have Renal Artery Stenosis, where the blood vessels supplying the kidneys narrow, tricking the kidneys into thinking blood pressure is low and triggering a massive hormonal surge to raise it. Obstructive Sleep Apnoea (OSA) is another frequent driver; the repeated drops in oxygen during sleep put the heart under immense stress, which manifests as stubborn daytime hypertension. Identifying these conditions requires a consultant's investigative eye and specialised testing.
Lifestyle and Interfering Substances
Sometimes the sabotage comes from your medicine cabinet or kitchen. Common over-the-counter medications, particularly non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, can significantly raise blood pressure and interfere with the effectiveness of your prescriptions. Similarly, high salt sensitivity or regular alcohol consumption can blunt the impact of even the most robust drug regimens. If you're concerned that your current tablets aren't hitting the mark, you might consider a specialist review to look for these hidden triggers and regain control over your cardiovascular health.
The Risks of Uncontrolled Hypertension: Beyond the Numbers
While the clinical definition of the condition focuses on medication counts, the actual reality of what is resistant hypertension is measured in the cumulative strain it places on your vital organs. When blood pressure remains uncontrolled over long periods, it accelerates atherosclerosis, the process where arteries harden and narrow due to plaque build-up. In resistant cases, this process isn't just steady; it's often accelerated. Data from 2017 to 2020 showed that 68.7% of those with hypertension had uncontrolled blood pressure, a statistic that highlights the scale of the challenge. This unyielding pressure creates a "target organ damage" profile that is significantly more complex than that seen in standard hypertension.
Heart Failure and Structural Changes
The heart is a muscle, and like any muscle, it adapts to a heavier workload. When forced to pump against the high resistance of narrowed or stiffened arteries, the walls of the left ventricle thicken. This condition, known as Left Ventricular Hypertrophy (LVH), might initially seem like a helpful adaptation, but it eventually makes the heart less flexible and less efficient. Over time, this structural change can lead to hypertensive heart failure, where the heart can no longer meet the body's demands. Dr Ayyaz Sultan, an experienced Consultant Cardiologist, uses advanced transthoracic echocardiograms to detect these early structural shifts. This allows for intervention before the damage becomes irreversible, shifting the focus from reactive treatment to proactive heart health management.
Kidney Function and Stroke Risk
The kidneys contain delicate filtration units called nephrons that are particularly sensitive to pressure. Uncontrolled hypertension acts like a pressure-cooker on these micro-vessels, eventually leading to chronic kidney disease or even renal failure. Similarly, the brain's small vessels are highly vulnerable. Persistent resistance increases the risk of Transient Ischaemic Attacks (TIAs) and major strokes, as the constant force can cause vessels to burst or become blocked. Beyond the brain, the aorta, which is the body's primary artery, can develop aneurysms under this relentless stress. Because resistant hypertension carries a higher cardiovascular risk than 'simple' hypertension, a proactive, specialist-led approach is essential to safeguard your long-term health. It's not just about lowering a number on a screen; it's about protecting the delicate systems that keep you alive.
Navigating the Diagnostic Journey: Specialist Investigations
Moving beyond the standard primary care setting is a critical step for anyone struggling to understand what is resistant hypertension in their own body. Whilst a GP provides excellent initial management, a specialist cardiac evaluation is designed to be an exhaustive investigation into why standard protocols have failed. This journey often begins with Ambulatory Blood Pressure Monitoring (ABPM), which is regarded as the gold standard for clinical accuracy. By wearing a portable cuff for 24 hours, we gather vital data on your 'dipping' patterns during sleep and your reactions to daily stressors. This provides a far more accurate profile than a single 'snapshot' reading in a clinic, helping us rule out the white coat effect once and for all.
The Transthoracic Echocardiogram
This non-invasive ultrasound scan is a cornerstone of our specialist toolkit. It allows us to visualise the heart's structure in real-time, specifically looking for evidence of Left Ventricular Hypertrophy (LVH), which we previously discussed as a structural consequence of long-term pressure. We measure the 'Ejection Fraction', which is a percentage representing how much blood the left ventricle pumps out with each contraction, to ensure the heart muscle remains strong and healthy. Additionally, we check the integrity of the heart valves, as issues like aortic stenosis can complicate blood pressure management and may require a different therapeutic approach altogether.
Advanced Diagnostic Screening
To look for secondary causes, we use the 'Plasma Aldosterone-to-Renin Ratio' alongside specific urine collections to check for hormonal triggers. These tests are the most effective way to identify hormonal resistance caused by overactive adrenal glands. If we suspect vascular issues, a Renal Artery Ultrasound or a Cardiac CT scan can check for narrowing of the arteries that supply the kidneys. We also utilise ECG and ambulatory monitoring to detect rhythm disturbances such as Atrial Fibrillation, which often coexists with high pressure. These investigations are not about 'over-testing' but about building a precise, evidence-based map of your unique cardiovascular health. If your blood pressure remains stubbornly high despite your best efforts, you can book a private consultation to begin this comprehensive diagnostic journey.
Personalised Management: A Consultant’s Approach to Care
When standard treatments reach their limit, the clinical focus must shift from broad protocols to the principles of precision medicine. For many patients, the emotional burden of "pill fatigue" is just as significant as the physical symptoms. It's common to feel a sense of failure when your readings don't improve, but understanding what is resistant hypertension helps reframe the situation. It isn't a failure of your effort; it's a sign that your unique physiology requires a more sophisticated, tailored strategy. One such approach is chronotherapy, where we optimise the timing of your medication, often moving certain doses to the evening to better manage the body's natural circadian rhythms and the early morning pressure surge.
If your blood pressure remains stubborn, we often introduce fourth-line agents or look toward cutting-edge pharmacological advancements. Spironolactone has long been a reliable choice, but newer options are expanding our toolkit. For instance, in March 2024, the medication aprocitentan was approved as the first hypertension drug with a novel mechanism of action in decades. We're also closely monitoring the progress of baxdrostat, a first-in-class aldosterone synthase inhibitor, with a regulatory decision expected in the second quarter of 2026. These developments, alongside device-based therapies like renal denervation, mean that even the most "untreatable" cases now have fresh avenues for management.
A Patient-Centred Treatment Plan
Dr Sultan’s approach is fundamentally holistic, recognising that hypertension often intersects with other complex conditions. For patients managing multi-system syndromes such as PoTS (Postural Tachycardia Syndrome) or those taking medication for ADHD, the management of blood pressure requires extreme precision. Some ADHD treatments can inadvertently raise pressure, whilst certain antihypertensives might exacerbate the lightheadedness associated with autonomic dysfunction. By organising care around these overlapping symptoms, we ensure that treating your blood pressure doesn't come at the cost of your overall well-being. Regular follow-up consultations allow us to fine-tune these complex regimes, ensuring they remain both effective and tolerable.
Next Steps: Booking a Private Consultation
Seeking a specialist second opinion is often the turning point for patients who have felt stuck in a cycle of uncontrolled readings. A private assessment provides the time and depth needed to move beyond the surface-level data. To prepare for your first visit, it's incredibly helpful to bring a one-week log of your home blood pressure readings and a comprehensive list of all current medications, including any over-the-counter supplements. This data allows us to hit the ground running. If you're ready to move beyond "standard care" and uncover the specific drivers of your condition, you can book a private cardiac consultation with Dr Sultan to investigate your hypertension and start your roadmap to better health.
Regaining Control Over Your Cardiovascular Health
Living with blood pressure that refuses to respond to standard treatment can feel like an exhausting uphill battle, but it's vital to remember that this resistance is a clinical signal rather than a permanent state. By moving beyond the broad protocols of primary care, we can uncover the specific secondary causes or physiological drivers that have kept your readings high. A specialist investigation isn't just about adding more pills; it's about precision, clarity, and protecting your vital organs from the cumulative strain of uncontrolled pressure.
Understanding what is resistant hypertension allows you to advocate for a deeper level of care that looks at your body as a whole. Dr Ayyaz Sultan, a Consultant Cardiologist since 2013 and a Fellow of the Royal College of Physicians (FRCP), specialises in these hard-to-treat and resistant conditions. He combines clinical mastership with a compassionate, patient-centred approach to help you navigate complex multi-system symptoms. You don't have to manage this uncertainty alone. With the right diagnostic roadmap and a personalised management plan, even the most stubborn readings can be brought under control. Take the next step toward peace of mind and Schedule a Specialist Cardiac Assessment with Dr Ayyaz Sultan today. Your heart health is a journey, and expert guidance can help you find the right path forward.
Frequently Asked Questions
Can resistant hypertension be cured or only managed?
Resistant hypertension can often be effectively reversed if a specific underlying "secondary" cause, such as a hormonal imbalance or a narrowed renal artery, is identified and treated. In cases where no single cause is found, the condition is managed through a meticulously tailored combination of medications and lifestyle shifts. Dr Sultan focuses on uncovering these treatable triggers to move beyond simply suppressing your symptoms with more pills.
Is it dangerous to take four or five different blood pressure tablets?
It's generally far safer to take a multi-drug regimen under specialist supervision than to leave high blood pressure uncontrolled. Each medication targets a different physiological system, such as the blood vessels, kidneys, or hormones, to achieve a cumulative effect that one drug alone cannot reach. Whilst taking several tablets may feel daunting, this evidence-based approach is the standard method for achieving cardiovascular stability in complex cases.
How do I know if my high blood pressure is caused by my kidneys?
Identifying kidney-related hypertension requires specific investigations such as a renal artery ultrasound or blood tests to check your glomerular filtration rate (GFR). Symptoms like changes in urination frequency or swelling in the ankles can sometimes occur, but renal issues are often "silent" and only detectable through testing. A specialist review is the most reliable way to determine if your renal health is the primary driver of your high readings.
What is the most common cause of resistant hypertension in the UK?
Primary aldosteronism, a condition where the adrenal glands produce too much of a salt-retaining hormone, is one of the most frequently identified medical causes of what is resistant hypertension in the UK. Beyond hormonal factors, lifestyle influences like high salt sensitivity and obstructive sleep apnoea are common contributors. Dr Sultan meticulously screens for these triggers to ensure your treatment plan addresses the actual root cause of the resistance.
Can stress alone cause resistant hypertension?
Whilst acute stress can cause temporary "spikes" in your readings, it's rarely the sole cause of true resistant hypertension. Resistance is typically driven by deep-seated physiological factors, such as hormonal imbalances or vascular stiffness, rather than just emotional pressure. However, chronic stress can certainly complicate your management, making a holistic approach that includes lifestyle support alongside medication essential for achieving long-term, stable control of your pressure.
What happens if Spironolactone doesn't work for my blood pressure?
If Spironolactone isn't effective or causes side effects, we explore alternative fourth-line agents or newer therapies like endothelin receptor antagonists. We might also consider device-based options such as renal denervation, which has been highlighted in the 2025 hypertension guidelines as a potential treatment for stubborn cases. The goal is always to find a precise combination of therapies that works for your specific biological profile and lifestyle needs.
Should I stop taking my supplements if I have resistant hypertension?
You shouldn't stop prescribed supplements without advice, but some over-the-counter products can inadvertently raise blood pressure or interfere with your medications. Substances like liquorice root or high doses of certain herbal extracts can sabotage your control. It's helpful to provide a full list of your supplements during your consultation so Dr Sultan can identify any potential interactions that might be contributing to your treatment resistance.
How often should I monitor my blood pressure at home if it's resistant?
For those managing what is resistant hypertension, we typically recommend monitoring your readings twice daily, once in the morning and once in the evening, for a full week before a specialist review. This provides a clear average that filters out daily fluctuations and the "white coat" effect. Once your regime is stable, Dr Sultan will advise on a less frequent, long-term monitoring schedule that ensures your safety without causing unnecessary anxiety.